Causes of Haemorrhoids
Several factors can increase the risk of developing haemorrhoids, including:
- Chronic constipation
- Frequent straining during bowel movements
- Poor dietary habits, especially a low-fibre diet
- Prolonged sitting
- Advancing age
- Pregnancy
- Liver cirrhosis and conditions causing increased abdominal pressure
Treatment for Internal Haemorrhoids
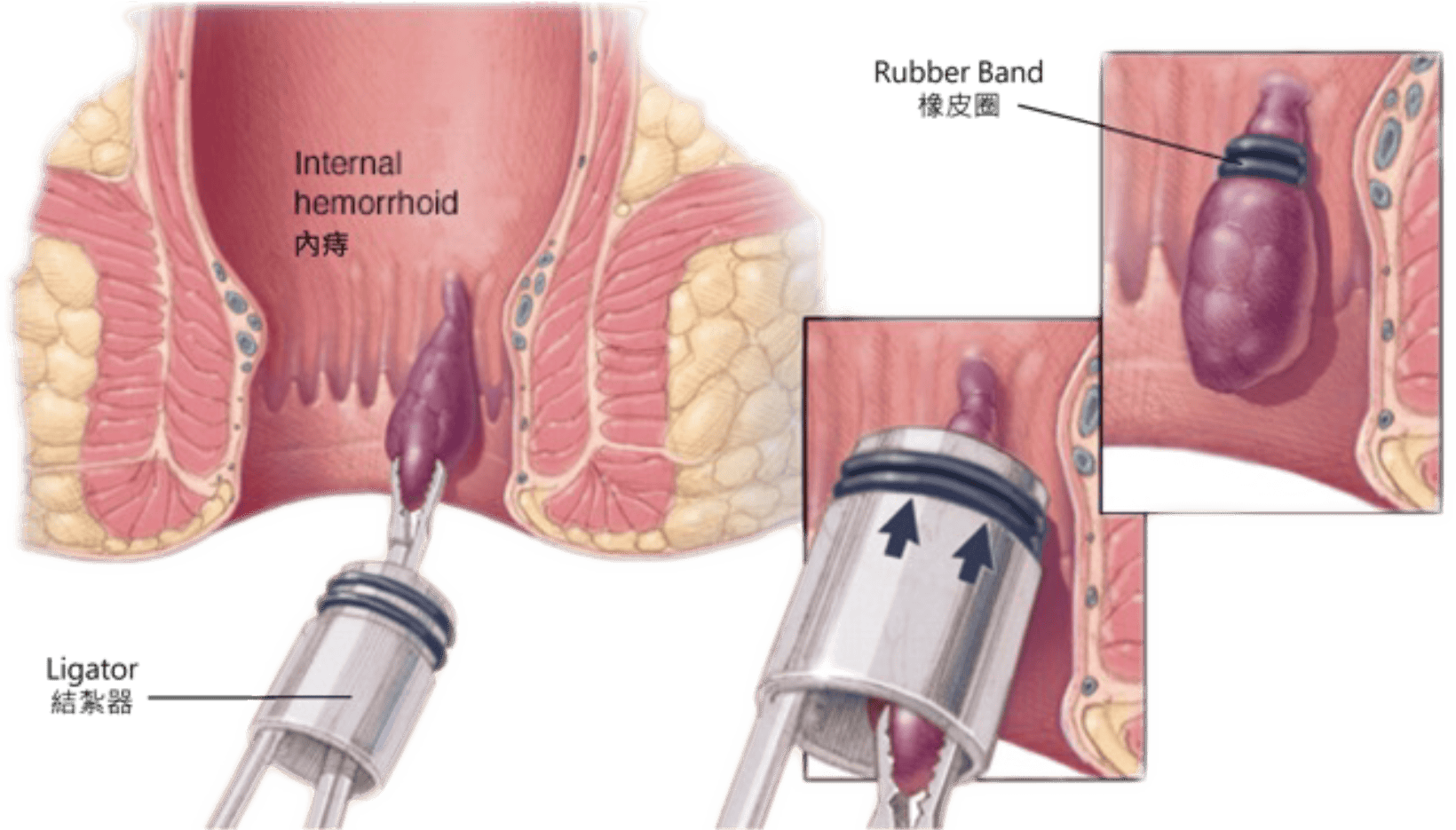
Rubber Band Ligation
A small rubber band is placed around the base of the haemorrhoid, cutting off its blood supply. The haemorrhoid gradually shrinks and falls off within a few days.
Suitable for: Grade I–III internal haemorrhoids.
Sclerotherapy Injection
A special sclerosing agent is injected into the haemorrhoid, causing it to shrink and scar.
Suitable for: Small internal haemorrhoids and patients unsuitable for surgery.
Stapled Haemorrhoidopexy
(Commonly known as the “Stapler Procedure” or PPH)
A circular stapling device is used to reposition prolapsed haemorrhoidal tissue and reduce its blood supply, causing it to shrink.
Advantages:
- Less postoperative pain
- Faster recovery
- Shorter hospital stay
Suitable for: Selected Grade II–III prolapsing haemorrhoids.
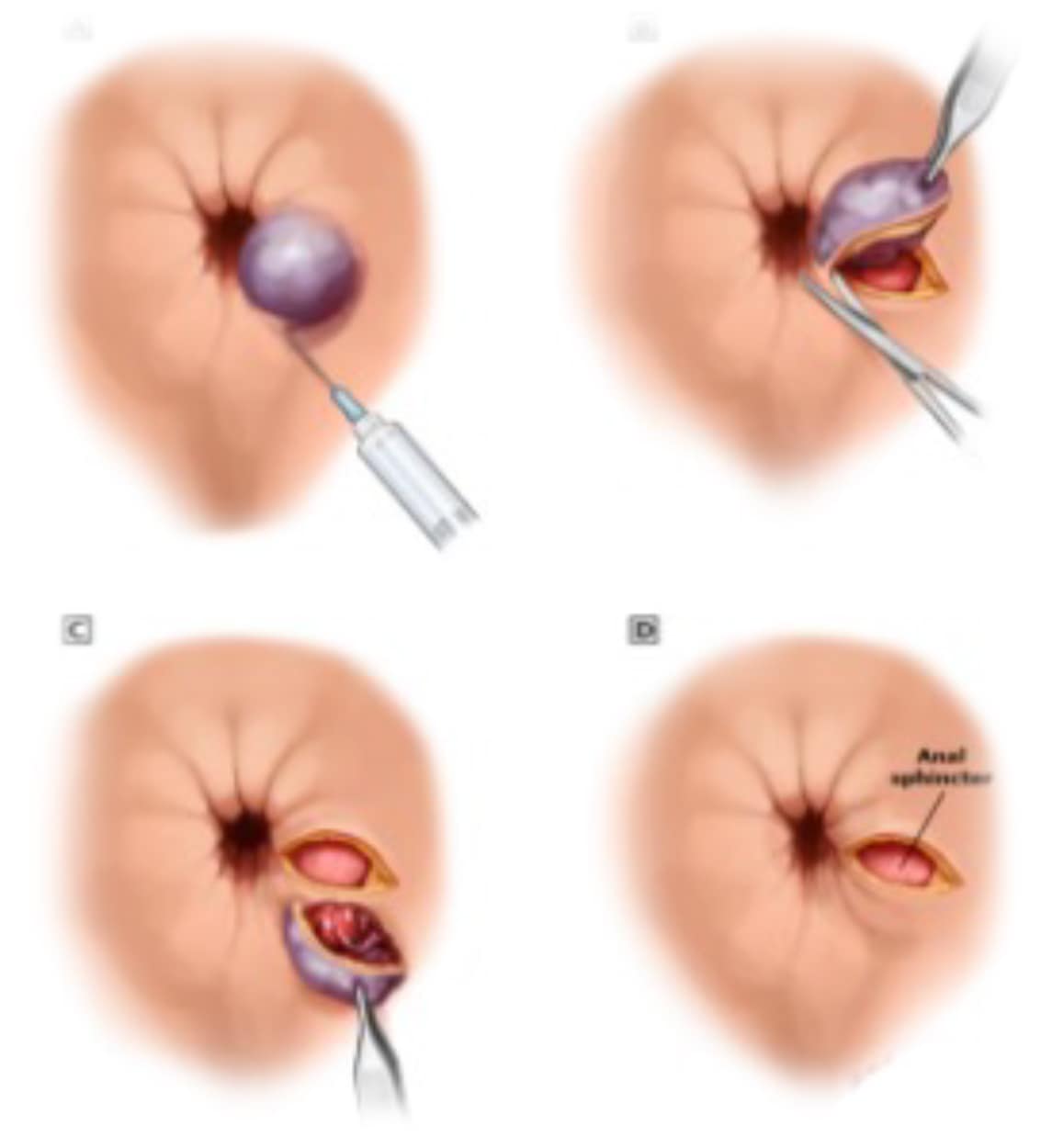
Treatment for External Haemorrhoids
Conventional Haemorrhoidectomy
A traditional surgical procedure to remove haemorrhoidal tissue.
Suitable for:
- Large external haemorrhoids
- Grade IV haemorrhoids
- Complex or recurrent cases
Stapled Haemorrhoidopexy (PPH)
May be suitable for selected patients with Grade I–III haemorrhoids and associated prolapse.
Types and Severity of Haemorrhoids
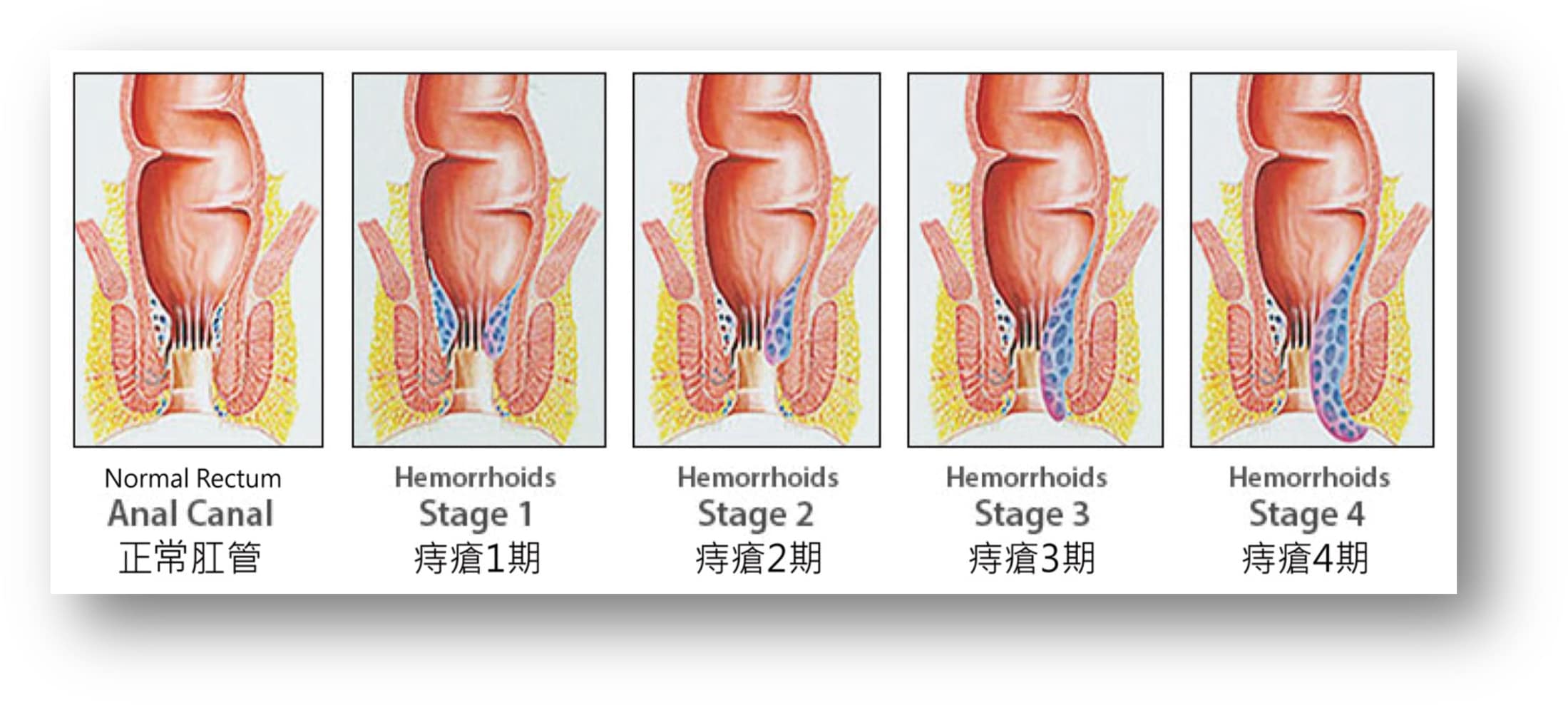
Grade I (Mild)
No visible prolapse
May cause painless rectal bleeding during bowel movements
Grade II (Moderate)
Haemorrhoids prolapse during bowel movements
Return spontaneously after defecation
Grade III (Moderately Severe)
Haemorrhoids prolapse during bowel movements
Require manual reduction (pushing back by hand)
Grade IV (Severe)
Haemorrhoids remain prolapsed permanently
Cannot be manually reduced
Often associated with pain, swelling, and complications